

Quick Links
The Aorta
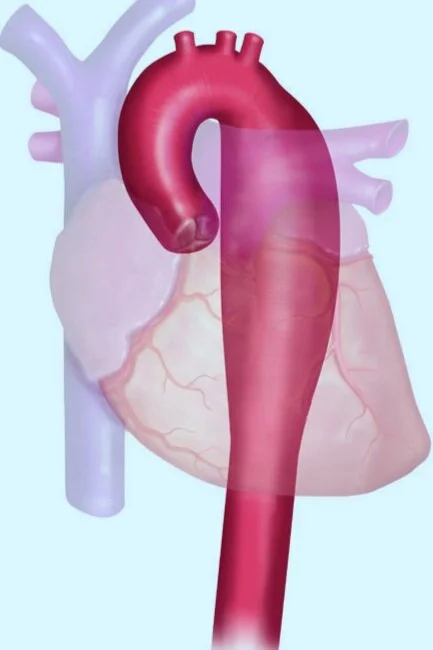
The human aorta is the main blood vessel that carries oxygen-rich blood from the heart to vessels that reach the head, neck, arms, legs and vital organs in the chest and abdomen. It is the largest artery in the body that arises from the left ventricle of the heart (aortic root), runs straight up (ascending aorta), bends over (aortic arch) and then runs down through the chest adjacent to the spine (descending thoracic aorta) and the abdomen (abdominal aorta) (figure 1) where it divides (aortic bifurcation) into the common iliac arteries that continues in to the legs (figure 2).
Figure 1: The Aorta
Figure 2
Structurally, the wall of the aorta has three layers, namely the intima, media and adventitia, which are comprised of smooth muscle and elastic fibres that function to withstand the pressure of blood flow.
Normal aortic diameter varies by location within the aorta, age, sex and body size. Various methods of imaging are used to examine the aorta and branch vessels and measure the size or diameter of the aorta. These imaging methods include transesophageal or transthoracic echocardiography, computed tomography (CT) with intravenous contrast and magnetic resonance imaging (MRI). Aortic measurements may differ depending on the imaging modality used, i.e. echocardiography measures the internal diameter whereas CT or MRI measures the external diameter, and thus measurements by CT/MRI are larger than measurements by echocardiography.
The aortic diameter normally increases with age and body surface area. At any given age, men typically have larger aortas than women. However, the aortic diameter may increase abnormally due to certain medical or lifestyle conditions leading to aortic disease.
Aortic Disease - Thoracic Aortic Aneurysms & Dissections (TAAD)
The human aorta can enlarge, dissect, rupture, develop atherosclerosis or become infected. Such aortic abnormalities are termed as aortopathies.
Aortic enlargement or dilation can cause the aortic valves to not fully close leading to back-flow of the blood from the aorta in to the heart termed as aortic regurgitation. This may cause forceful heartbeats and shortness of breath during normal light activity.
An aortic aneurysm is a permanent, localized enlargement of the aorta to more than 50% of its normal diameter.
Clinically, two predominant spatial distribution of aortic aneurysms have been observed: thoracic aortic aneurysms (TAA) and abdominal aortic aneurysms (AAA).
A thoracic aortic aneurysm (TAA) is a permanent, localized enlargement anywhere in the thoracic aorta (located above the diaphragm): the aortic root, ascending aorta, aortic arch (Figure 3a) and/or the descending aorta (Figure 3b).
Figure 3a: Aortic Arch Aneurysm
Figure 3b: Descending Thoracic Aortic Aneurysm
Abdominal aortic aneurysms (AAA) are located under the diaphragm and often occur between the renal arteries and the aortic bifurcation.
Most patients with TAAs usually have no symptoms (asymptomatic) at the time of diagnosis. Some patients may develop symptoms due to compression of the aneurysm against adjacent structures, aortic regurgitation or with serious life-threatening complications such as aortic dissection or rupture.
An aortic dissection (or tear) is defined as a disruption of the medial layer of the aorta resulting in bleeding within and along the wall of the aorta and separation of the layers of the wall of the aorta. Although most aortic dissections are preceded by an aneurysm, some dissections can occur without significant enlargement of the aorta.
Aortic dissections can be classified by the Stanford criteria, based on the involvement of the ascending aorta, as follows:
1) Type A dissections: involve the ascending aorta regardless of the point of origin and may or may not extend to the descending thoracic aorta. Acute type A dissections are associated with life-threatening complications (such as rupture and cardiac tamponade) and often require emergency surgery of the aorta.
2) Type B dissections: originate in the descending thoracic aorta and extend down the descending thoracic aorta or abdominal aorta. Type B dissections do not involve the ascending aorta. Type B aortic dissections are often treated medically unless life-threatening complications develop.
Depending on where the dissection occurs and how much it spreads, an aortic dissection may extend to or block the arteries to the brain, kidneys, heart, arms, or legs, and result in complications in these organs. (IRAD online). Aortic dissections are fatal because they decrease blood flow to the different parts of the body such as the brain and other vital organs and eventually ruptures the aorta, leading to extensive blood loss and death.
Risk Factors of Aortic Dissection
Hypertension, age, weight lifting, physical trauma, smoking, use of cocaine or other powerful stimulants.
Genetic syndromes such as bicuspid aortic valve, Turner syndrome, inflammatory diseases of the aorta, and Heritable thoracic aortic disease (HTAD) / genetic aortic disorders (GAD) such as; Marfan syndrome, Loeys-Dietz syndrome, vascular Ehlers-Danlos syndrome and familial thoracic aortic aneurysms and dissection (FTAAD).
Heritable thoracic aortic disease (HTAD) refers to thoracic aortic disease in patients and families in whom there is a confirmed gene mutation (genetic aortic disorder) or at least a strong suspicion for a genetic factor based on clinical features or family history (and hence heritable) that confers a high risk for thoracic aortic aneurysms and dissections (TAAD). Learn More
Prior cardiac surgery or catheterization is also a risk factor for aortic dissection.
Symptoms
Aortic dissections and/or aneurysms may present with the following symptoms. However, some patients have confessed that they did not have any symptoms before or at the time of a dissection.
severe, sharp pain in the chest, back or abdomen
pain in the jaw and neck radiating into arms and head
sudden pain in the throat
difficulty breathing or speaking
dizziness and/or nausea
weak or unusual blood pressure
loss of consciousness
weakness of limbs
numbness in one or more limbs
vision disturbances
other symptoms similar to a stroke or heart attack
Management
Management of thoracic aortic aneurysm and/or dissection requires:
A multidisciplinary team of specialists familiar with HTAD, including a clinical geneticist, cardiologist, and cardiothoracic and vascular surgeons.
Imaging (echocardiography, CT, MRI) for early detection and surveillance of aortic aneurysms
Medical therapy using beta adrenergic-blocking agents (e.g. atenolol), Losartan, Angiotensin-II Receptor Blockers (ARBs) or Angiotensin-converting Enzyme (ACE) inhibitors
Elective surgery to repair an aneurysm and prevent an aortic dissection.
Genetic testing to identify the cause of HTAD and cascade testing to identify other relatives at risk for TAAD. Depending on the underlying genetic condition, results of genetic testing can guide aortic and other vascular surveillance and timing of elective surgical repair of aortic aneurysms to prevent a dissection or rupture.
Women with aortic disease or predisposition to aortic disease have an increased risk for aortic dissection and other complications during pregnancy. Some antihypertensive medications cannot be taken during pregnancy due to a high risk of birth defects and fetal loss. Women should discuss these risks with her cardiologist before getting pregnant. Women should consult with a genetic counselor regarding inheritance, risk to offspring, and genetic testing options. Pregnant women with aortic disease should be closely monitored by her cardiologist and high-risk obstetrician-gynecologist and undergo periodic imaging of the aorta throughout the pregnancy and postpartum.
Lifestyle modifications such as avoidance of smoking, strenuous resistive (isometric) exercises (i.e. heavy weightlifting or weight training), cocaine and other powerful stimulants.
References